

Longshore and Harbor Workers Compensation
TL;DR: This is a summary of the LS-203 blog post
- The LS-203 form is used to file workers’ compensation claims under U.S. laws such as the Longshore and Harbor Workers’ Compensation Act (LHWCA), Defense Base Act, and others.
- The form gathers detailed personal, employment, and injury-related information across 36 sections to process claims efficiently.
- Key fields include the claimant’s name, injury date, occupation, wages at the time of injury, and details about the accident, such as location and medical treatment.
- It is important to complete the form thoroughly, as missing information could lead to a denied claim. Legal assistance can help ensure accuracy and increase the chances of receiving benefits.
- The form must be submitted to the U.S. Department of Labor for processing and eligibility verification.
The LS-203 Form titled “Employee’s Claim for Compensation,” issued by the U.S. Department of Labor, Office of Workers’ Compensation Programs. This form, identified with OMB Control Number 1240-0014 and revised in November 2023 and Expires: 11/30/2026, is used by employees to file claims for compensation under various acts including the Longshore and Harbor Workers’ Compensation Act, Defense Base Act, Outer Continental Shelf Lands Act, and Nonappropriated Fund Instrumentalities Act.
If you are searching for an experienced Louisiana Longshore Harbor Death Benefits Workers Compensation lawyer near you, contact Charles Lavis at (504) 684-7331 for a free consultation and Lavis Law Firm can help you with your LS-203 form.
On This Page:
ToggleLS203 Form
The LS-203 provides a detailed structure ensuring that the form collects essential information required to efficiently process workers’ compensation claims under various U.S. laws. It is designed to gather detailed personal, employment, and injury-related information to accurately determine benefits and legal compliance.
If you’re eligible for benefits under the Longshore and Harbor Workers’ Compensation Act (LHWCA), you’ll need to file an LHWCA claim in Louisiana using the U.S. Department of Labor Form LS-203. Complete the form carefully, as missing any required information could result in a denied claim. While you may file Form LS-203 independently, many workers find it beneficial to work with a maritime injury lawyer to navigate the process and secure benefits.
The LS-203 form requires detailed information across 36 sections, with only two fields that may be left blank. All other sections must be accurately completed to qualify for LHWCA benefits. The specific questions are outlined below. Our longshore lawyer can help you get the longshore workers’ comp settlement you deserve. Be sure to file an LHWCA claim in Louisiana.
How To File the LS-203 Form
A New Orleans longshore accident lawyer specializes in helping workers navigate the complexities of filing claims after an injury at the workplace. When a longshoreman is injured, the form LS-203 is required to report the accident, and it is essential for filing a compensation claim under workers’ compensation laws. This official form documents the injury severity, details medical treatment, and includes supporting medical and employment details. It is a mandatory step in claim submission to ensure that injured workers are eligible for benefits and compensation. Lawyers assist in completing and submitting the form, documenting the injury, and ensuring that it is filled out with accurate and detailed information. Lavis Law Firm can help verify the details, handle any discrepancies, and address issues that might arise during the claims process.
The New Orleans longshore accident lawyer ensures that the form is completed promptly, a key factor in avoiding delays in the compensation process. Our office can also assist in ensuring that the workers’ rights are protected and help in resolving disputes that may arise. We investigate the accident to ensure that the form includes all necessary information about the accident investigation and injury assessment. Our lawyer helps workers understand how to submit their forms correctly and address any potential penalties for submitting them late. In addition, these lawyers help the injured worker navigate the legal documentation required for compensation, including determining how much benefits the worker is entitled to based on the accident’s severity and the compensable injuries sustained.
Why It’s Important to Have a Longshore Harbor Accident Lawyer In Your Corner
For the worker, it is vital to have a supportive lawyer who can ensure that all necessary documentation is in place. A skilled lawyer will complete and file the form in compliance with legal standards, ensuring the injured worker gets the workers’ compensation they deserve. They also manage communication between the worker and the employer, helping the worker understand their eligibility for disability or long-term compensation. The lawyer’s experience in maritime law helps workers understand the legal nuances of the workers’ compensation system, the maritime laws involved, and how to best protect their interests. They are also crucial in guiding injured workers through the documentation process, ensuring the claim is not delayed or denied due to missing details.
From the perspective of an injured worker, having a lawyer who understands the compensation process and can manage the timely processing of the claim offers peace of mind during a difficult time. The lawyer is committed to ensuring the worker’s eligibility for benefits is accurately assessed, and the process of claim submission is as smooth as possible. For the employer, it is equally important to ensure the form is filed correctly to avoid complications or penalties. Legal professionals also play a role in supporting both the worker and employer by offering advice on how to handle claims appropriately and verify the information needed for the compensation process.
A New Orleans longshore accident lawyer is the guide injured workers need to navigate the legal complexities of longshore accidents, ensuring that every aspect of the claim is completed and submitted with accuracy. With their knowledge of maritime law, workers’ compensation, and claim processing, they ensure that the injured worker is not only compensated but also supported throughout the process, offering a clear, comprehensive, and timely approach to accident reporting and compensation.
LS-203 Form Questions
- OWCP No.: Assigned Office of Workers’ Compensation Programs number for the claim if one has already been assigned
- Carrier’s No.: Insurance carrier’s number associated with the claim.
- Name of Person Making Claim: Full name of the claimant (first, middle initial, last).
- Date of Injury: Specific date on which the injury occurred.
- Claimant’s Address: Full residential address of the claimant.
- Marital Status: Marital status of the claimant, either married or single.
- Gender Identity: Claimant’s gender identity from provided options or an option to decline to answer.
- Date of Birth: Claimant’s date of birth.
- Social Security #: Mandatory field for the claimant’s Social Security Number.
- a. Nationality: The claimant is asked to specify their nationality. This information could be relevant for understanding jurisdictional and legal considerations, especially in cases involving international or immigrant workers.
- Did Injury Cause Loss of Time Beyond Day or Shift of Accident?: Yes/no question regarding time loss due to the injury.
- Date and Time of Accident: Exact date and time when the accident took place.
- a. Did You Stop Work Immediately?: This is a yes/no question designed to establish the immediate impact of the injury. It asks whether the claimant stopped working immediately after the accident, providing insights into the severity of the incident and its immediate effects on the claimant’s ability to continue working.
- Date and Hour Pay Stopped: When the claimant stopped receiving their regular pay due to the injury.
- Date and Hour You Returned to Work: Date and time when the claimant resumed work, if applicable.
- Occupation (Job Title): Job title of the claimant at the time of injury.
- Injured While Doing Regular Work?: Whether the injury occurred while performing regular job duties.
- Wages or Earnings When Injured: Weekly earnings and total earnings in the year immediately before the injury.
- Has 3rd Party or Other Claim Been Made Because of This Injury?: Information on whether any third-party claims have been made due to the injury.
- Number of Years You Worked for This Employer: Duration of employment with the current employer.
- Number of Days Usually Worked Per Week: Average number of days worked per week.
- Name of Supervisor at Time of Accident: Supervisor’s name at the time of the injury.
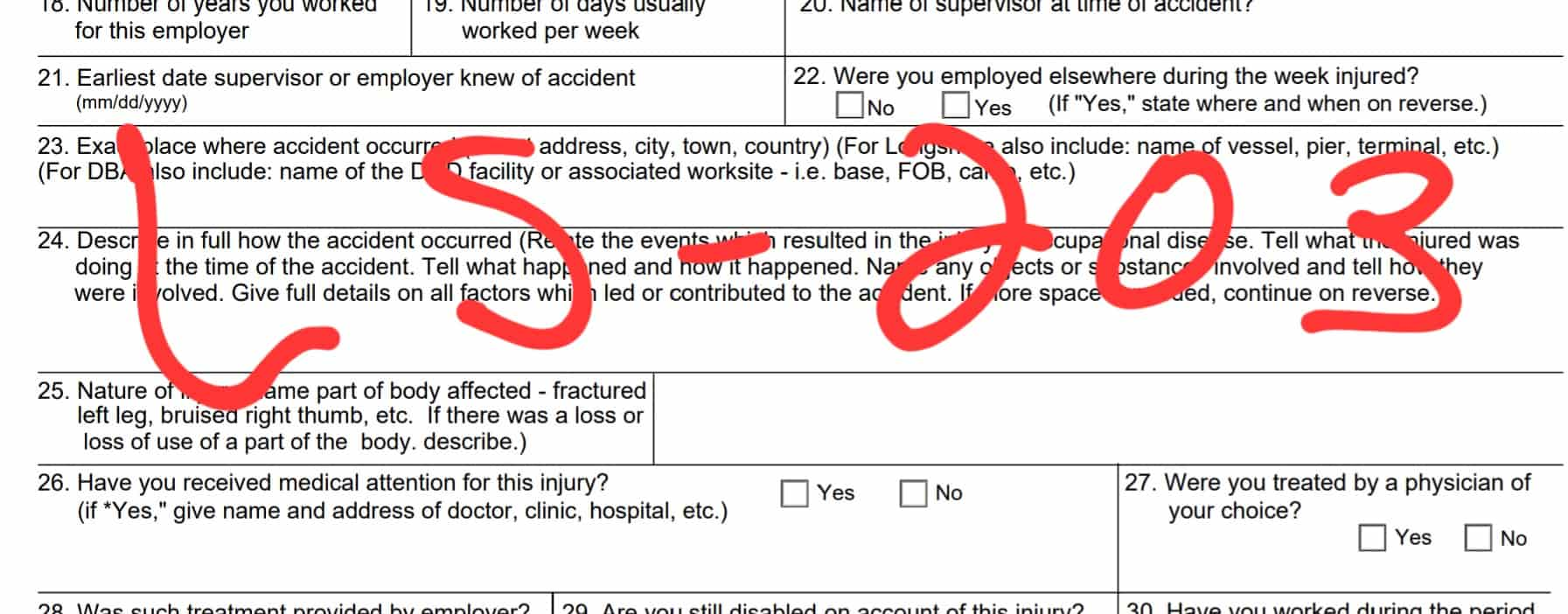
- Earliest Date Supervisor or Employer Knew of Accident: When the employer or supervisor first became aware of the accident.
- Were You Employed Elsewhere During the Week Injured?: Employment status elsewhere during the week of the injury.
- Exact Place Where Accident Occurred: This section requires a detailed description of the specific location where the accident took place. The description should include:
- – Street Address: The precise street address where the accident occurred.
- – City, Town, Country: These details help pinpoint the location within broader geographical boundaries.
- – Additional specific details for certain types of claims:
- – For Longshore Claims: It is necessary to include the name of the vessel (if applicable), the pier, and the terminal where the incident occurred. These details are crucial for incidents related to maritime operations and help in identifying the exact maritime location, which can be significant in the context of maritime law.
- – For Defense Base Act (DBA) Claims: The name of the Department of Defense (DOD) facility or associated worksite needs to be specified, such as a base, Forward Operating Base (FOB), camp, etc. This provides clarity on the military or defense context of the accident, which is essential for claims under the DBA that covers civilian employees working on military bases or under a contract with the U.S. government for public works or for national defense. Lavis Law Firm has helped injured workers with Defense Base Act PTSD settlements and hearing loss. Contact us today.
- Describe in Full How the Accident Occurred: Comprehensive description of how the accident happened, including activities at the time of the accident, factors contributing to the accident, and involved objects or substances.
- Nature of Injury: Detailed description of the injury and affected body parts.
- Have You Received Medical Attention for This Injury?: Status of medical attention received, with provider details if applicable.
- Were You Treated by a Physician of Your Choice?: Indicates if the treatment was by a physician chosen by the claimant.
- Was Such Treatment Provided by Employer?: Whether the employer provided the medical treatment.
- Are You Still Disabled on Account of This Injury?: Current disability status due to the injury.
- Have You Worked During the Period of Disability?: Queries whether the claimant has engaged in any form of work during the period they were deemed disabled due to the injury.
- Have You Received Any Wages Since Becoming Disabled?: Seeks to know if the claimant has received any wages or compensation after they became disabled, which is important for adjusting potential benefits.
- Has Injury Resulted in Permanent Disability, Amputation or Serious Disfigurement?: Asks the claimant to disclose if the injury has led to permanent disability, amputation, or any serious disfigurement, which can significantly affect the type and duration of benefits received.
- Name of Employer (Individual or Firm Name): Requires the full legal name of the employer at the time of the accident.
- Nature of Employer’s Business: Describes the type of business or industry in which the employer operates, relevant for understanding the work environment and potential hazards.
- Address of Employer: The complete address of the employer, necessary for official communications and potential investigations.
- If an Accident Occurred Outside the U.S., State Whether You Are a U.S. Citizen: This is particularly crucial for determining jurisdiction and the applicability of U.S. workers’ compensation laws if the accident occurred abroad.
- I Hereby Make a Claim for Compensation Benefits: The claimant’s formal declaration of their intent to seek compensation benefits, which must be signed to process the claim.
- Date of This Claim: The date when the claim form is completed and submitted,
This detailed structure ensures that the form collects all essential information required for the efficient processing of workers’ compensation claims under various U.S. laws. The form MUST also be properly delivered to the US Department of Labor.
Download The LS-203 Form
Filing a claim for benefits under the Longshore and Harbor Workers’ Compensation Act requires providing extensive information. If you have questions about completing Form LS-203 or need assistance with your claim, contact us today for expert support.
Below you can download a PDF of the LS203 form.
You can also find our Louisiana workers’ compensation forms here.
Contact a LHWCA Claims Louisiana Longshore Accident Lawyer Near You Today
